Vitreomacular Traction Syndrome (VMT)
Vitreomacular traction syndrome (VMT) occurs when the vitreous gel inside the eye partially separates from the retina but remains abnormally attached to the macula, the central portion of the retina responsible for detailed vision. This persistent pulling or “traction” can distort the macula and lead to blurred or distorted vision.
Some cases of VMT resolve on their own, while others require treatment to preserve or improve vision. Early diagnosis and close monitoring by a retina specialist can help determine the most appropriate course of action.
What Is the Vitreous and Macula?
The vitreous is the clear, gel-like substance that fills the center of the eye. As we age, the vitreous naturally shrinks and separates from the retina in a process called a posterior vitreous detachment (PVD).
The macula is the central part of the retina responsible for:
- Reading vision
- Recognizing faces
- Seeing fine details
- Color vision
- Driving and other tasks requiring sharp central vision
Normally, the vitreous separates completely from the retina. In VMT, part of the vitreous remains attached to the macula, creating abnormal traction.
What Causes Vitreomacular Traction?
VMT most commonly develops as part of the normal aging process.
Risk factors include:
- Increasing age
- Female sex
- High myopia (nearsightedness)
- Previous inflammation inside the eye
- Diabetic retinopathy
- Retinal vein occlusion
- Prior retinal surgery
- Epiretinal membranes
The severity of symptoms depends on the amount of traction and whether other retinal conditions are present.
What Are the Symptoms?
Some patients have no symptoms and are diagnosed during a routine examination.
When symptoms occur, they may include:
Blurred Central Vision
Objects may appear less sharp than usual.
Distorted Vision (Metamorphopsia)
Straight lines may appear bent, wavy, or distorted.
Difficulty Reading
Patients often notice trouble with small print.
Reduced Visual Quality
Vision may seem hazy or less crisp.
Central Blind Spots
In more advanced cases, small missing areas in central vision can develop.
Symptoms usually affect one eye initially but may occur in both eyes.
What Complications Can Occur?
Persistent vitreomacular traction can lead to additional retinal problems, including:
Macular Hole
Ongoing traction may create a full-thickness opening in the macula.
Cystoid Macular Edema
Fluid accumulation within the retina can worsen vision.
Epiretinal Membrane
Scar tissue may form on the retinal surface.
Progressive Vision Loss
Untreated traction can lead to worsening distortion and reduced visual function.
How Is VMT Diagnosed?
A retina specialist uses a combination of examination findings and retinal imaging.
Dilated Retinal Examination
The retina is evaluated for:
- Vitreous attachment
- Macular abnormalities
- Epiretinal membranes
- Macular holes
- Other retinal conditions
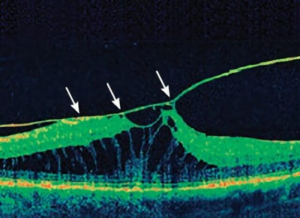
Optical Coherence Tomography (OCT)
OCT is the most important test for diagnosing VMT.
It provides detailed cross-sectional images of the retina and can show:
- Persistent vitreous attachment
- The degree of traction
- Retinal distortion
- Cystic changes
- Early or full-thickness macular holes
OCT is also used to monitor progression and response to treatment.
Amsler Grid Testing
An Amsler grid may help patients monitor for changes in central vision at home.
How Is Vitreomacular Traction Treated?
Treatment depends on the severity of symptoms and the amount of traction present.
Observation
Patients with mild symptoms and minimal traction may simply be monitored.
Because some cases resolve spontaneously, your retina specialist may recommend:
- Periodic examinations
- Repeat OCT imaging
- Home monitoring with an Amsler grid
Pars Plana Vitrectomy
Vitrectomy surgery is the most established treatment for symptomatic VMT.
During surgery:
- The vitreous gel is removed.
- Traction is released from the macula.
- Associated epiretinal membranes may also be peeled if present.
Many patients experience improvement in visual distortion and stabilization or improvement of vision.
Pharmacologic Vitreolysis
Pharmacologic vitreolysis is no longer frequently used for this condition. Historically, ocriplasmin was approved for this purpose. However, it is no longer widely available or commonly used in clinical practice due to variable outcomes and concerns regarding side effects.
Your retina specialist will discuss whether observation or surgery is most appropriate for your individual situation.
What Is the Prognosis?
The outlook for VMT is generally favorable.
Many patients experience:
- Stable vision with observation
- Spontaneous release of traction
- Improvement after surgery
Visual outcomes depend on:
- How long traction has been present
- Whether a macular hole has developed
- The degree of retinal damage before treatment
- The presence of other retinal diseases
Earlier intervention in appropriate cases may improve the likelihood of visual recovery.
Living With Vitreomacular Traction
If you have VMT:
- Attend all scheduled follow-up visits.
- Report worsening distortion or vision loss promptly.
- Use an Amsler grid as instructed.
- Ask your retina specialist about changes noted on OCT imaging.
- Continue monitoring even if symptoms improve.
Understanding your condition can help you recognize changes early and preserve your vision.
Frequently Asked Questions (FAQ)
Will vitreomacular traction go away on its own?
Sometimes. Mild cases can spontaneously release as the vitreous completes its separation from the retina. Other cases persist and may require treatment.
Is surgery always necessary?
No. Many patients can be safely observed. Surgery is generally reserved for patients with bothersome symptoms, worsening traction, or associated complications.
Can VMT cause a macular hole?
Yes. Persistent traction on the macula can sometimes lead to the development of a full-thickness macular hole, which may require surgical repair.