Acquired Vitelliform Lesions
Acquired vitelliform lesions (AVLs) are yellowish deposits that develop beneath the center of the retina, called the macula. The macula is responsible for sharp central vision needed for reading, driving, and recognizing faces. AVLs are sometimes called adult-onset vitelliform maculopathy or adult pattern dystrophy. These lesions are usually found in adults in their 40s, 50s, and beyond.
Although the name sounds complicated, AVLs are often slow-moving conditions. Many patients maintain useful vision for years, and some may never notice major symptoms. However, regular monitoring by a retina specialist is important because AVLs can sometimes resemble or coexist with other retinal conditions such as age-related macular degeneration (AMD).
What Causes Acquired Vitelliform Lesions?
AVLs develop when yellow material made up of waste products from light-sensing retinal cells builds up beneath the retina. This material collects between the retina and a support layer called the retinal pigment epithelium (RPE).
Doctors do not fully understand why these deposits form, but they may be related to aging changes in the retina or problems with how retinal cells process waste material. AVLs can occur alone or alongside conditions such as:
- Age-related macular degeneration (AMD)
- Drusen (small yellow deposits under the retina)
- Pattern dystrophies
- Epiretinal membranes
Unlike inherited Best disease, AVLs usually appear later in life and are not commonly linked to a strong family history.
Symptoms
Some patients have no symptoms at all and learn about the condition during a routine eye exam. Others may notice:
- Blurred central vision
- Distorted vision (straight lines appearing wavy)
- Difficulty reading
- Mild reduction in color perception
- A small blurry spot in the center of vision
Peripheral (side) vision is usually not affected.
Vision can vary widely among patients. Many people maintain driving vision for years.
How Are AVLs Diagnosed?
A retina specialist can often recognize AVLs during a dilated retinal examination. Several imaging tests may be used to confirm the diagnosis and monitor changes over time.
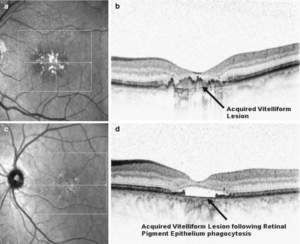
Optical Coherence Tomography (OCT)
OCT is one of the most important tests for AVLs. It creates detailed cross-sectional images of the retina and helps show the yellow material beneath the macula.
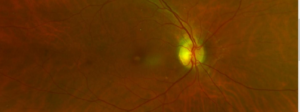
Fundus Photography
Retinal photographs may show a round yellow lesion beneath the center of the retina as shown in the photograph below.
Additional Imaging
Your retina specialist may also perform:
- Fundus autofluorescence imaging
- Fluorescein angiography
- OCT angiography
These tests help distinguish AVLs from wet macular degeneration or abnormal blood vessel growth.
Treatment
In many cases, AVLs do not require immediate treatment. Instead, careful observation with regular retinal examinations and OCT imaging is recommended.
It is important to correctly diagnose AVLs because they can sometimes look similar to wet AMD. Wet AMD often requires anti-VEGF eye injections, while uncomplicated AVLs usually do not.
Some AVLs remain stable for many years. Others may gradually shrink or disappear over time. Unfortunately, when the deposits resolve, some patients develop thinning or scarring of the retina (atrophy), which can reduce central vision.
If abnormal blood vessels develop beneath the retina — a complication called choroidal neovascularization — treatment with anti-VEGF injections may become necessary.
Prognosis
The outlook for patients with AVLs is often reasonably good. Many patients keep functional reading and driving vision for years. Vision loss, when it occurs, is usually gradual rather than sudden.
Regular follow-up appointments are important because the condition can change over time. Monitoring allows your retina specialist to detect complications early and recommend treatment if needed.
Frequently Asked Questions (FAQ)
Are acquired vitelliform lesions the same as macular degeneration?
Not exactly. AVLs can resemble age-related macular degeneration and may occur alongside AMD, but they are different conditions. Proper retinal imaging is important to distinguish between them.
Can acquired vitelliform lesions cause blindness?
AVLs rarely cause complete blindness because peripheral vision is usually preserved. However, they can affect central vision used for reading and detailed tasks.
Do acquired vitelliform lesions need injections?
Most AVLs do not require injections. However, if abnormal blood vessels develop beneath the retina, anti-VEGF injections may be recommended.